Beyond Roughness: How MATRIX Dual® Creates Multi-Scale Implant Surfaces for Enhanced Osseointegration
By: Craig Rosenblum, Himed President
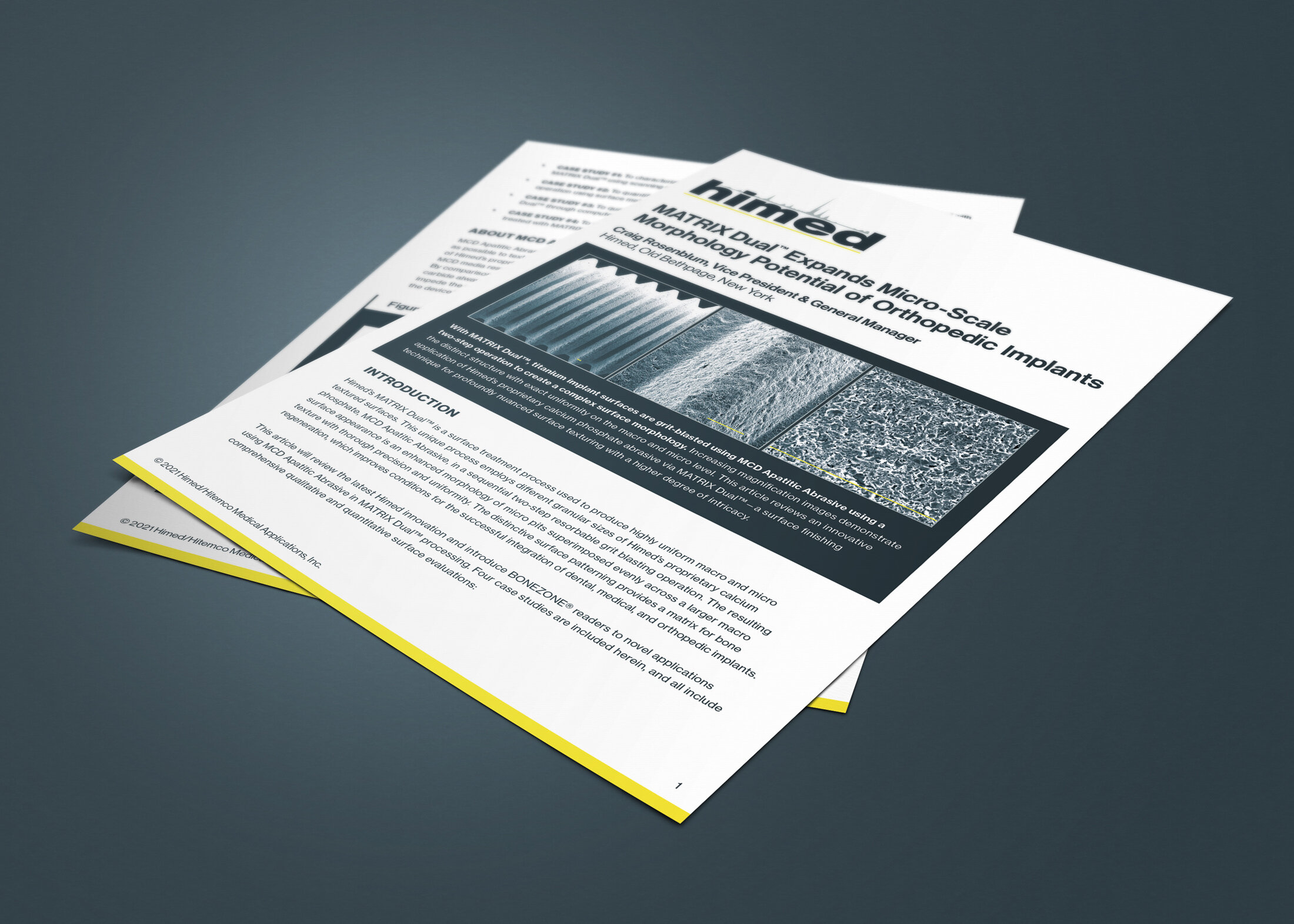
Expanding implant possibilities with complex surface topography
When a medical implant is placed into bone, the first interactions occur at the implant–tissue interface. Surface texture influences how proteins adsorb to the implant, how osteoblasts attach and proliferate, and how new bone forms during the healing process. (1–4)
Decades of research have shown that moderately rough implant surfaces consistently outperform smooth, machined ones by promoting stronger bone-to-implant contact and better mechanical fixation. (1–4) Consequently, surface roughening has become a standard part of many dental, orthopedic, and spinal implant manufacturing processes.
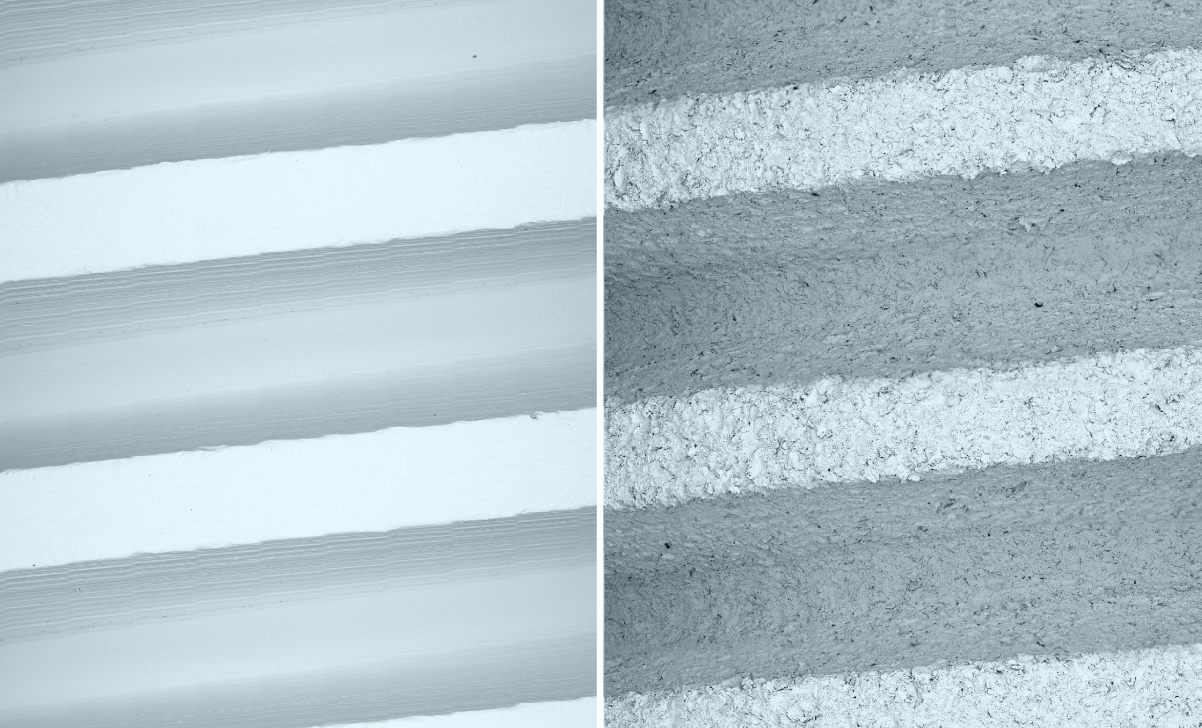
A scanning electron microscope (SEM) image at 750x magnification showing the relatively smooth surface texture of an untreated threaded stainless steel implant manufactured through conventional machining (left), and the same surface after post-processing with Himed’s proprietary MCD apatitic abrasive (right). The treated surface shows no significant material loss during micro grit blasting, but now exhibits a surface topography more conducive to osseointegration.
Additionally, researchers have increasingly recognized that a surface property like roughness (Ra) can provide a range of biomimetic customizations to further enhance implant performance. After all, natural bone is a highly complex material with many variations in structural features at different scales, from larger architectural elements to micro- and nano-scale topographies that affect cellular behavior. (5)
This realization has driven interest in multi-scale implant surfaces—engineered topographies that combine different levels of surface texture to create a more biologically active interface. Emerging evidence suggests these multi-scale surfaces may support both mechanical integration and cellular signaling more effectively than single-scale surface modifications alone. (5–7)
However, as implant manufacturers pursue increasingly sophisticated surface designs, they must naturally contend with how to create complex multi-scale textures consistently, precisely, and at a production scale.
Creating complex surface morphology with MATRIX Dual®
MATRIX Dual® is Himed's advanced surface treatment technology designed specifically to create highly uniform multi-scale surface morphologies on a variety of medical implant substrates, including titanium, titanium alloys, medical polymers such as polyetheretherketone (PEEK), and 316L stainless steel.
Unlike a single-step grit blasting process, MATRIX Dual® uses a sequential two-stage operation with different particle sizes of Himed's proprietary MCD Apatitic Abrasive. The first stage establishes a controlled macro-textured surface, while a second blasting step develops distinct micro-scale features evenly spread across the larger surface area. (17)
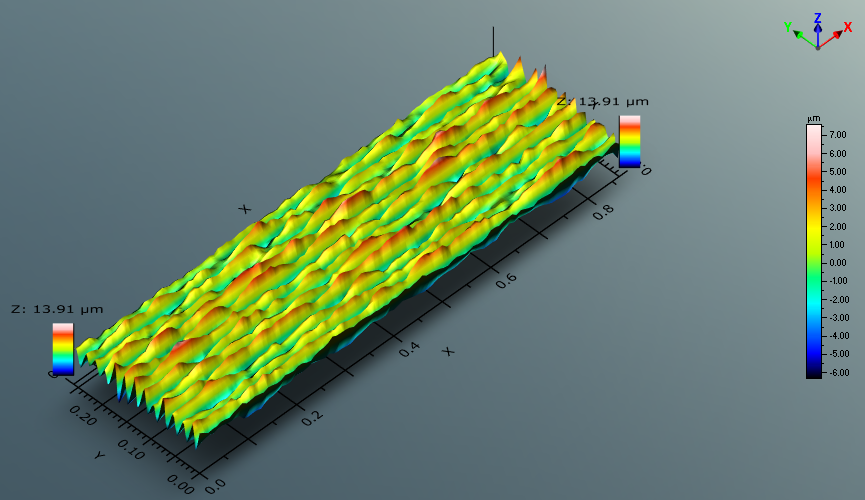
A 3D surface profile topography of a titanium coupon post-processed using the two-step MATRIX Dual® micro-blasting process, generated and analyzed with TrueGage Surface Metrology software that enables non-contact optical analysis of the surface. The multi-scale surface offers both macro and micro topography, with a high degree of overall uniformity across the entire area and an average combined Ra range of 1.3–1.7 µm.
The result is a highly uniform surface architecture that combines macro- and micro-scale textures in a single, tightly controlled process. Instead of depending on random surface variation, MATRIX Dual® allows manufacturers to create repeatable, application-specific surface characteristics tailored to their performance goals. (17)
Importantly, this secondary micro-texturing is achieved mechanically rather than through aggressive chemical modification. While other implant post-processing methodologies rely on acid etching to generate finer-scale features, chemical treatments can introduce additional process variability and may unfavorably alter previously established macro-scale topography. (20) MATRIX Dual® instead develops its hierarchical morphology through consistently applied sequential blasting operations, providing greater control over the final surface architecture. (17)
Implant surface roughness and biological response
The biological response to an implant surface is influenced by more than a single roughness value. Moderately rough surfaces, typically in the 1–2 µm Ra range, have consistently demonstrated favorable outcomes for osseointegration by balancing enhanced biological activity with long-term implant stability. (2,4,16) Within this Ra range, implant surfaces promote protein adsorption, osteoblast attachment, and mechanical interlocking between bone and implant. (1,2,8–10,12)
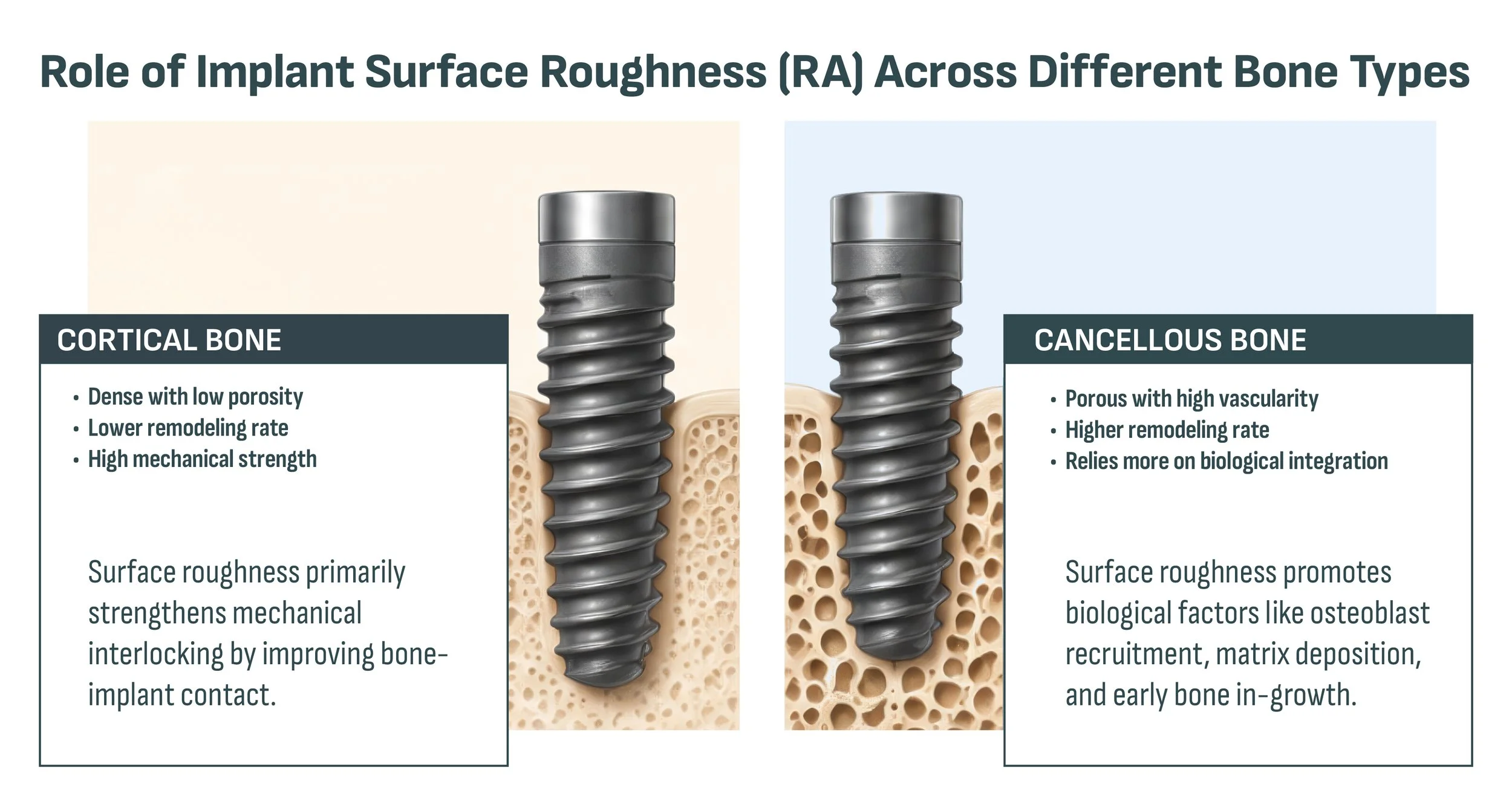
While current research indicates that a 1–2 µm Ra range for implant surfaces remains optimal across bone types, differences in native bone density and porosity between cortical and cancellous bone can impact whether mechanical or biological factors play a larger role in improving osseointegration.
Excessively rough surfaces, by contrast, can pose challenges. Increased surface irregularities may encourage bacterial adhesion and biofilm formation, especially in dental applications, while extreme roughness might affect fatigue behavior or cause localized stress concentrations. (13–15)
Complex surface architectures seek to optimize this balance by introducing multiple scales of topography rather than simply increasing roughness. Micro-scale features contribute to mechanical fixation, while smaller-scale surface structures may further influence protein interactions and cellular signaling pathways associated with bone formation. (5–7)
For implant developers, the objective is not simply to create a rougher surface, but to create a more functional one, which may require biomimetic surface characteristics more analogous to the type of bone receiving the implant.
The advantage of resorbable blast media (RBM)
The effectiveness of MATRIX Dual® starts with the abrasive itself. MCD Apatitic Abrasive is a proprietary, multi-phase calcium phosphate media designed specifically for medical device surface texturing. Unlike conventional grit-blasting materials such as aluminum oxide or silicon carbide, MCD is both biocompatible and resorbable.
Traditional blasting media can leave residual particles embedded in an implant surface after processing. These residues may affect biological performance, introduce localized stress concentrations, or complicate subsequent surface treatments. (13) MCD was developed to address these concerns. Following processing and passivation, implants treated with MCD display exceptionally clean textured surfaces while removing minimal substrate material, helping preserve fine micro-threads, porous lattice structures, and other precision-engineered features. (17–18)
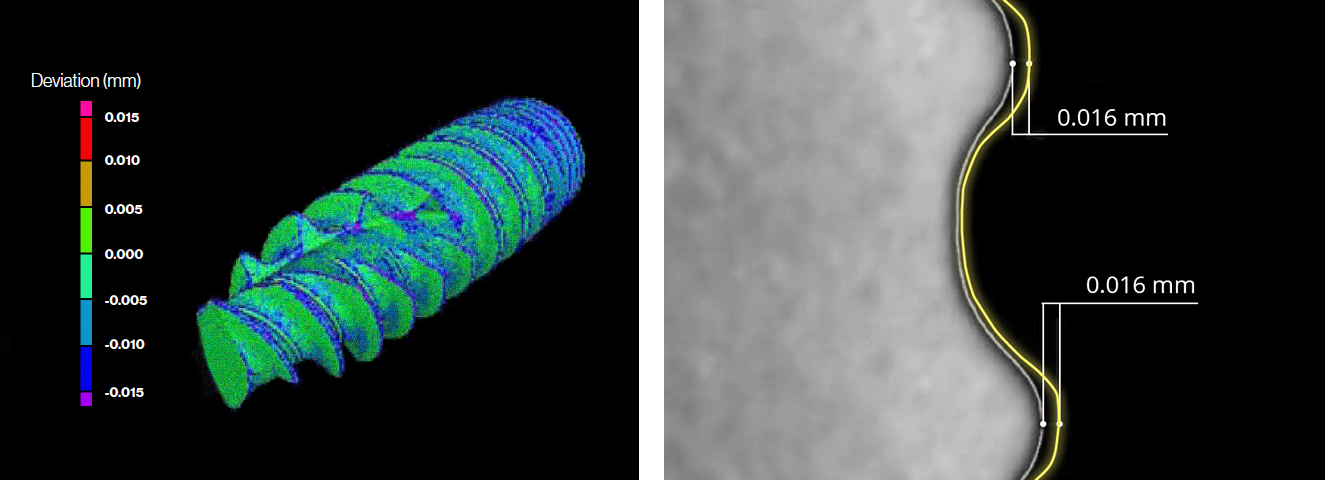
Computed tomography renderings subsequent to MATRIX Dual® surface treatment along an entire spinal implant body (left) showing an insignificant overall reduction of 7–16 µm in material along the implant diameter (right, with the yellow line showing the pre-treatement dimension, and the gray line after treatment).
Available in a range of particle sizes, MCD also offers a high degree of process flexibility, allowing surface textures to be tailored to specific application requirements while maintaining dimensional accuracy. Whether used as a final surface treatment or as a precursor to additional coating technologies, MCD provides a level of control that extends well beyond conventional blasting media.
Precision, Repeatability, and Manufacturing Control
Sophisticated surface designs are only useful if they can be consistently reproduced. To ensure repeatability, MATRIX Dual® is performed using Himed's Fully Automated Blasting System (FABS), a robotic plasma-spray platform specifically developed for post-processing medical devices. The system allows precise control over process variables and ensures highly reproducible surface results across both development and production environments. (19)
For implants needing selective treatment, custom masking fixtures can precisely define treated and untreated areas. This enables manufacturers to apply specific surface textures only where required, while safeguarding critical functional features such as precision threads or mating surfaces. (19)
The process has been validated under ISO 13485:2016 quality system requirements and filed with the FDA under Master Access File (MAF) 1239.
Engineering the Next Generation of Implant Surfaces
As implant design advances, manufacturers are increasingly shifting from basic roughness targets toward more sophisticated surface structures aimed at actively promoting osseointegration.
Research continues to show the value of combining multiple topography scales to influence both mechanical fixation and cellular behavior. (5-7) However, achieving these benefits requires manufacturing processes that can produce complex surface morphologies with precision and consistency.
MATRIX Dual® was developed to meet that challenge. By combining a biocompatible, resorbable abrasive, automated process control, and a unique two-stage texturing method, MATRIX Dual® allows implant manufacturers to create highly engineered multi-scale surfaces while ensuring the repeatability and dimensional accuracy needed for modern medical device production.
For developers seeking greater control over implant surface performance, MATRIX Dual® offers a practical pathway beyond conventional roughening techniques and toward the next generation of implant surface engineering.
MATRIX Dual® White Paper
Interested in taking a closer look at data specific to the MATRIX Dual® process? Request a download of our white paper that details four case studies which use advanced scanning technology to characterize—at the submicron and nanoscale level—implant surfaces treated with this two-step process.
References
Buser D, Schenk RK, Steinemann S, Fiorellini JP, Fox CH, Stich H. Influence of surface characteristics on bone integration of titanium implants. J Biomed Mater Res. 1991;25(7):889-902.
Wennerberg A, Albrektsson T. Effects of titanium surface topography on bone integration: a systematic review. Clin Oral Implants Res. 2009;20(Suppl 4):172-184.
Jemt T, Olsson M, Franke Stenport V. Incidence of first implant failure: a retroprospective study of 27 years of implant operations at one specialist clinic. Clin Implant Dent Relat Res. 2015;17(Suppl 2):e501-e510.
Mustafa K, Wennerberg A, Wroblewski J, Hultenby K, Lopez BS, Arvidson K. Determining optimal surface roughness of TiO₂ blasted titanium implant material for attachment, proliferation and differentiation of cells derived from human mandibular alveolar bone. Clin Oral Implants Res. 2001;12(5):515-525.
Gittens RA, Olivares-Navarrete R, Schwartz Z, Boyan BD. Implant osseointegration and the role of microroughness and nanostructures: lessons for spine implants. Acta Biomater. 2014;10(8):3363-3371.
Wu Y, Zhang X, Li H, et al. Research progress on surface modification of titanium implants. Coatings. 2025;15(2):229.
Șerbănescu CM, Popa CL, Predoi D. Nanofeatured titanium surfaces for dental implants: a systematic evaluation of osseointegration. Antibiotics (Basel). 2025;14(12):1191.
Deligianni DD, Katsala N, Ladas S, Sotiropoulou D, Amedee J, Missirlis YF. Effect of surface roughness of the titanium alloy Ti-6Al-4V on human bone marrow cell response and on protein adsorption. Biomaterials. 2001;22(11):1241-1251.
Zhao G, Schwartz Z, Wieland M, Rupp F, Geis-Gerstorfer J, Cochran DL, Boyan BD. High surface energy enhances cell response to titanium substrate microstructure. J Biomed Mater Res A. 2005;74(1):49-58.
Mishra D, Bernhardt A, Gelinsky M, Basu B. Human osteoblast-derived biochemical cues and microsurface topography modulate osteogenesis in vitro and in vivo. Biointerphases. 2025;20(5):051002.
Zhang M, Liu S, Xing J, et al. Graphene oxide-modified PEEK composites: properties and applications in orthopaedic repair - a review. J Orthop Translat. 2025;56:101028.
Ma JY, Zhou X, Yao ZH, et al. Biomimetic titanium implant surface modified with magnesium-containing nanowires to promote osseointegration: in vitro and in vivo investigations. Colloids Surf B Biointerfaces. 2026;262:115555.
Teughels W, Van Assche N, Sliepen I, Quirynen M. Effect of material characteristics and surface topography on biofilm development. Clin Oral Implants Res. 2006;17(Suppl 2):68-81.
Tardelli JDC, Bagnato VS, Reis ACD. Bacterial adhesion strength on titanium surfaces quantified by atomic force microscopy: a systematic review. Antibiotics (Basel). 2023;12(6):994.
Sumner DR. Long-term implant fixation and stress-shielding in total hip replacement. J Biomech. 2015;48(5):797-800.
Albrektsson T, Wennerberg A. Oral implant surfaces: Part 1—review focusing on topographic and chemical properties of different surfaces and in vivo responses to them. Int J Prosthodont. 2004;17(5):536-543.
Himed Test Study—2017. Data on file at Himed.
Himed Test Study—2018. Data on file at Himed.
Himed Test Study—2020. Data on file at Himed.
Al-Radha ASD. The influence of different acids etch on dental implants titanium surface. IOSR J Dent Med Sci. 2016;15(8):87-91.
About the Author

Craig Rosenblum
PRESIDENT, HIMED LLC
Craig Rosenblum has worked for over a decade at Himed LLC, a global leader in calcium phosphate biomaterials with over 35 years of innovation in plasma spray coatings and surface treatments for medical and dental devices. He collaborates with manufacturers worldwide to deliver advanced biomaterial solutions, with a focus on hydroxyapatite-based bioceramics.
Craig holds both a BS and MS in Materials Science & Engineering (Biomaterials) from The Johns Hopkins University. He has been a featured speaker at a variety of conferences, including the Orthopaedic Manufacturing & Technology Exposition and Conference (OMTEC), the Society for Biomaterials, and the International Conference for Materials Science and Engineering.
NOTE: Every effort has been made to ensure the accuracy of the information shared in this post at the time of publication. This content is not intended as medical advice and should not be used in place of consultation with a qualified healthcare provider. If you believe any part of this post is inaccurate or could benefit from an update, please contact us.